
Schwartz Rounds: Pre‑Event Psychosocial Risk Management Through Collective Reflection
Pre-Event Psychosocial Risk Management Framework 8

Introduction
Every day, millions of people go to work carrying more than tools and laptops. They take with them the weight of decisions that affect lives, the emotional labour of caring for others, the fatigue of constant vigilance and the moral conflicts that arise when ideals collide with reality. By 2025 nearly half of the workers reported feeling stressed every day and more than 80% felt they were on the brink of burnout[1]. Nurses now report the highest stress levels of any healthcare profession[2] and the moral injuries they experience have become so common that a whole field of research is devoted to understanding them[3]. These stresses do not dissipate at the end of a shift; they accumulate and can manifest as anxiety, depression, reduced performance and staff turnover.
Psychological harm at work is not always visible. Psychosocial hazards – things that can harm someone’s mental health – include job demands, low job control, poor support, lack of role clarity, inadequate reward or recognition, poor organisational justice, remote or isolated work, violence and aggression, bullying, harassment and traumatic events[4]. Safe Work Australia warns that these hazards often interact; high workloads become more damaging when workers cannot take breaks or when no one is around to help[5]. The consequences are real. In Australia there has been a 56% increase in serious workers’ compensation claims for assault and workplace violence over the last five years[6].
Yet the most insidious psychosocial hazards are not captured by injury reports or surveillance systems. They live in the stories workers tell themselves when they go home: the patients they could not save, the cruelty they witnessed, the colleagues who left, the fear of speaking up. Addressing these hazards requires more than policies and checklists; it requires making the invisible visible and creating spaces where people can process what they experience before it becomes harm. This is the domain of pre‑event psychosocial risk management – proactively addressing psychological hazards before they lead to injury.
The Growing Imperative for Psychosocial Risk Management
Pre‑event psychosocial risk management is becoming a statutory and moral necessity. Under Australia’s model Work Health and Safety (WHS) laws, persons conducting a business or undertaking (PCBUs) must manage the risk of psychosocial hazards and have regard to matters such as job demands, poor support and harmful behaviours[8]. Failure to meet these duties carries significant penalties and exposes organisations to compensation claims.
Beyond compliance, organisations that ignore psychosocial hazards face tangible business costs. High stress levels lead to decreased productivity, increased errors, absenteeism and turnover. One 2025 workplace study found that toxic cultures and unrealistic workloads were among the leading causes of chronic stress[9]. In healthcare, burnout has been linked to lower patient satisfaction and increased medical errors. Evidence from the 2024 Well‑Being Index shows that nurses who perceive their workplace as supportive of their well‑being are more engaged and healthier[10]. Proactive psychosocial risk management is therefore both a legal obligation and a strategic necessity.
Theoretical Foundations: Emotional Labour, Moral Injury and Psychological Safety
Emotional Labour and Burnout
Sociologist Arlie Hochschild introduced the concept of emotional labour to describe the requirement for workers to manage their feelings to fulfil a job role. Professions such as healthcare, regulation, social services and law enforcement demand sustained emotional labour – empathising with clients while suppressing personal reactions. Over time, this leads to burnout, a syndrome characterised by emotional exhaustion, depersonalisation and a sense of reduced personal accomplishment. Burnout undermines the capacity to care and increases the risk of mistakes. Creating space for staff to express and process emotions is therefore a fundamental control for psychosocial risk.
Moral Distress and Moral Injury
Moral distress occurs when individuals know the ethically appropriate action to take but are prevented from doing so because of organisational or resource constraints. Repeated exposure to such situations can lead to moral injury, a deep psychological wound that arises when actions or events transgress a person’s moral code. A 2026 review of moral injury in healthcare workers notes that the COVID‑19 pandemic intensified exposure to morally transgressive events (e.g., patients dying without family, resource shortages) and that addressing moral injury requires organisational change, training and peer support initiatives[3]. Without mechanisms for processing these experiences, moral injury contributes to depression, post‑traumatic stress and occupational turnover.
Psychological Safety and Collective Processing
Harvard researcher Amy Edmondson defines psychological safety as a shared belief that it is safe to take interpersonal risks. Psychological safety enables speaking up about risks, reporting concerns and learning from failure. Teams with high psychological safety exhibit greater trust, openness and adaptability. Social support is one of the most protective factors against workplace stress and psychological harm, yet in many organisations support is fragmented or informal. Collective processing – coming together to reflect on shared experiences – reduces isolation, normalises emotional responses and strengthens relational systems.
Enter Schwartz Rounds: Making the Invisible Visible
Schwartz Rounds began in the United States through the Schwartz Center for Compassionate Healthcare and have since been adopted by more than 900 healthcare organisations across the U.S., Canada, the UK, Ireland, Australia and New Zealand[11]. The program provides a regular open forum for multidisciplinary discussion of the psychosocial and emotional aspects of caring for patients and families[12]. Each session is organised around a compelling patient story and includes clinical and non‑clinical panelists and participants[13]. Unlike clinical morbidity and mortality meetings, the focus is not on technical analysis or performance but on what the experience felt like, how it affected individuals and teams and what meaning participants derived from it.
Core Characteristics
Focus on Emotional and Relational Experience – Schwartz Rounds avoid problem‑solving and instead encourage participants to explore their emotional responses. This shift from performance to experience normalises vulnerability and reduces stigma around emotional expression.
Multidisciplinary Participation – Staff from different roles, disciplines and levels of the organisation attend. This diversity breaks down silos and fosters empathy across hierarchical boundaries.
Facilitated, Non‑Judgemental Dialogue – Trained facilitators ensure conversations remain respectful, confidential and blame‑free. Psychological containment enables the safe discussion of emotionally charged topics.
Core Components of Schwartz Rounds
These sessions typically built around three key components.
1. A Real Case
A panel presents a real scenario that carried emotional or ethical complexity.
This may include:
· A difficult patient interaction
· Exposure to trauma
· Conflict between professional values and organisational constraints
· A situation involving loss, error, or uncertainty
The authenticity of the case is essential. It anchors the discussion in lived experience.
2. Facilitated Reflection
Facilitators guide participants to explore:
· Emotional responses
· Relational impacts
· Ethical tensions
Importantly, discussion is not directed toward problem-solving or performance evaluation.
This creates space for reflection rather than judgement.
3. Collective Insight
Participants connect the case to their own experiences.
This process:
· Reduces isolation
· Builds empathy
· Reinforces shared understanding
Over time, this strengthens organisational cohesion.
By design, the process is pre‑event: it occurs regardless of whether a critical incident has occurred, allowing staff to process cumulative exposure rather than waiting for harm to emerge.
Virtual Rounds and New Modalities
The COVID‑19 pandemic accelerated innovation in psychosocial support. The New Jersey Nursing Emotional Well‑Being Institute (NJNEW) launched Virtual Schwartz Rounds in 2020. These one‑hour sessions use two facilitators to guide discussions where nurse panelists share stories around a theme; they are conducted over Zoom and provide anonymity for participants[14]. As of 2026, NJNEW had hosted 99 sessions for more than 6000 nurses[15]. The program emphasises compassion, connection and community, offering nurses an opportunity to discuss social and emotional issues amid fast‑paced, stressed work lives[16]. Topics have included “Am I Ever Off Duty? The Emotional Weight of Nursing” and “Thriving on the Night Shift: Intentional Self‑Care for Healthy Habits”[17], illustrating the breadth of concerns that merit reflection.
Evidence for Impact
Schwartz Rounds have been the subject of more than two decades of international research. A 2018 evaluation across over 140 National Health Service (NHS) organisations found significant reductions in psychological distress, improved coping with emotional demands and increased perceived organisational support among participants. Subsequent studies reported reductions in emotional exhaustion and compassion fatigue and improved psychological safety.
Research Summary
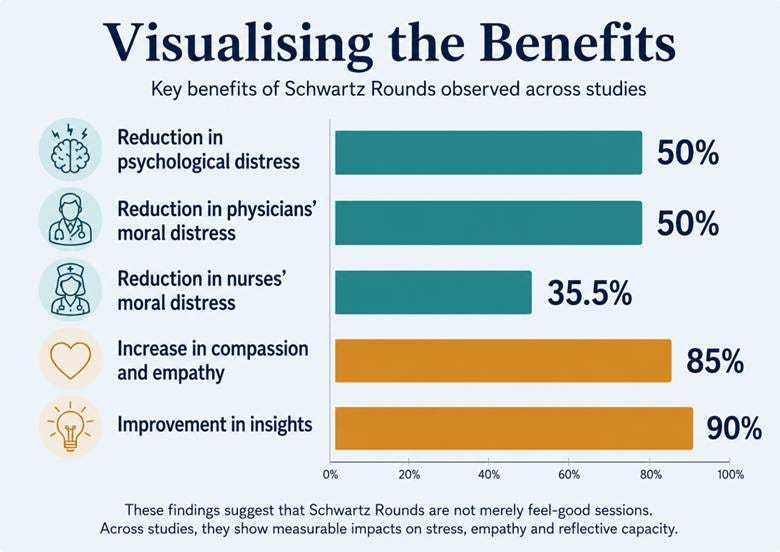
The Schwartz Center summarises results from more than 100 peer‑reviewed and descriptive studies. Compared with non‑attendees, individuals who participate in Schwartz Rounds report a 50% reduction in psychological distress, reduced moral distress (50 % of physicians and 35.5 % of nurses), increased confidence in handling sensitive issues, decreased isolation and an 85%–90% increase in compassion, empathy and insights[18]. The impact is cumulative: the more sessions attended, the greater the benefits[19]. At the team level, studies note improved teamwork, more openness to offering and receiving support, and a flattening of hierarchy[20].
Visualising the Benefits
Virtual Schwartz Rounds Research
Emerging evidence suggests that virtual adaptations are effective and complement other forms of support. A 2026 cross‑sectional survey of 235 nurses who participated in the NJNEW Virtual Schwartz Rounds examined whether participation influenced engagement in other well‑being programs. The study found that nurses who joined workplace well‑being programs were more likely to use external resources for emotional support – such as spending time with animals, mindfulness practices, community groups and counselling[21]. In other words, participation in a formal program did not replace self‑care or community support; it catalysed a multipronged approach to well‑being[22]. This aligns with the Grossman health production model, which argues that investments in emotional well‑being increase an individual’s overall stock of health and the efficiency of future investments[23].
Moral Injury and Peer Support
The 2026 review on moral injury in healthcare workers highlighted that addressing moral injury requires organisational change, training and peer support initiatives[3]. Schwartz Rounds satisfy the peer support element by creating a safe space for collective reflection. They also generate insights that leaders can use to inform organisational change and training. By acknowledging morally injurious events and facilitating open discussion, Rounds help mitigate the risk of long‑term psychological harm.
Intersections with Psychosocial Risk Management
Schwartz Rounds directly address several categories of psychosocial hazards identified by Safe Work Australia. Emotional demand and exposure to distress are inherent to healthcare and high‑risk professions. Rounds provide a structured outlet for processing these experiences, reducing cumulative emotional load. By validating ethical tensions and moral conflicts, they help mitigate moral injury. Through cross‑functional participation, they reduce interpersonal strain and silos. The visible investment in reflective practice signals organisational support, countering perceptions of neglect or indifference. Finally, by normalising help‑seeking, Rounds reduce stigma around mental health and encourage workers to seek formal and informal support.
The program’s strengths align with the WHS framework for managing psychosocial hazards. Safe Work Australia’s risk management process involves identifying hazards, assessing risks, implementing controls and reviewing their effectiveness[24]. Schwartz Rounds contribute to several of these steps:
· Hazard identification – Themes emerging from Rounds highlight hidden pressures, ethical dilemmas and interpersonal tensions that may not appear in surveys or incident reports.
· Risk assessment – Sharing lived experience provides context on the severity and likelihood of harm. For example, repeated stories about unsustainable caseloads signal high job demands and low control.
· Risk control – Rounds themselves function as a control by reducing isolation and supporting coping. They also inform improvements such as workload adjustments, training and resource allocation.
· Review and improvement – Analysing recurring themes and participation rates helps organisations monitor psychosocial risks over time and evaluate the effectiveness of interventions.
Broader Trends and the Hierarchy of Controls
While healthcare has been a proving ground for psychosocial interventions, rising stress and trauma exposure across the broader workforce highlight why such controls are essential. The Australian Psychological Services report on emerging trends notes that 59 % of Australians experienced at least one personal stressor in the last twelve months, and an estimated 75 % have experienced a traumatic event at some point in their lives[25]. People with a mental health condition were more likely to have encountered stressors (68 %) than those without a condition (52 %)[25]. These statistics underscore that psychosocial risk is a population‑level issue, not confined to extreme occupations.
Workplace behaviours compound these exposures. Of approximately 10 000 serious mental stress claims in 2021–22, the highest proportion (27.5 %) were attributed to work‑related harassment and bullying[26]. National surveys suggest compensation data underestimates the problem; 41 % of women reported being sexually harassed at work in the last five years[27]. Meta‑analytic evidence shows that organisational factors such as high job demands, role ambiguity, role conflict and work constraints are stronger predictors of bullying exposure than individual traits like self‑esteem[28]. Conversely, job resources such as autonomy and clarity decrease the likelihood of harassment[29]. In other words, psychosocial harm is driven by how work is designed and managed, not by the perceived resilience of workers.
Recognising this, leading safety agencies promote a hierarchy of psychosocial controls akin to the hierarchy used for physical hazards. The Australian Psychological Services framework identifies four tiers across the employee lifecycle[30]:
· Promote – Enhance connection and purpose with work and the organisation to create healthy, supportive systems. This includes fostering a culture of compassion and connection so that work is experienced as meaningful.
· Prevent – Eliminate or reduce known psychosocial hazards through primary interventions that directly influence the psychosocial environment. Examples include redesigning jobs to balance demands and resources, clarifying roles, improving change management and addressing harmful behaviours.
· Early Intervention – Enhance how individuals and teams respond to stressors and support one another. Schwartz Rounds sit within this tier. They do not eliminate hazards themselves but equip workers with coping mechanisms, surface hidden pressures and inform organisational change.
· Support – Provide timely, person‑centred support to treat, compensate and rehabilitate employees who experience psychological injury. This includes access to counselling, peer support, return‑to‑work programs and compensation when harm occurs.
This hierarchy underscores that pre‑event controls like Schwartz Rounds are necessary but not sufficient. Organisations should view reflective forums as part of a layered strategy: combining promotion of positive culture, primary prevention of hazards, secondary interventions for early response and tertiary support for those harmed. Boards and executives have a role to play – the report emphasises leadership education, infrastructure reviews and capability building[31]. Maturity assessments help organisations evaluate their current controls and identify gaps across the hierarchy. By integrating Rounds with broader risk management and leadership development, organisations can move from reactive to proactive psychosocial safety.
Implementation Guidance: Making Rounds Work
Implementing Schwartz Rounds effectively requires treating them as a structured organisational intervention, not a discretionary wellness activity. The following considerations are critical:
1. Pre-Implimentation
Facilitator capability is paramount. Facilitators must be trained in psychological safety, group dynamics and managing emotional disclosure. The Schwartz Center emphasises that trained facilitation is essential to maintain safety and effectiveness[18]. Without skilled facilitators sessions can devolve into complaint forums or disengagement.
Assess organisational readiness. Levels of trust, psychological safety and openness vary. In low‑trust environments participation may be superficial or avoided. Building trust may require smaller pilot groups or parallel initiatives to foster safety. Leadership commitment must be visible; leaders should attend Rounds without defensiveness and demonstrate that reflection is valued.
Align with regulatory requirements. Map the themes of Rounds to WHS risk categories to demonstrate due diligence. Where recurring issues relate to job demands or poor support, ensure that risk registers and prevention plans are updated accordingly.
Leadership commitment must be visible and behavioural. Leaders should participate without defensiveness and reinforce that reflection is valued. Evidence from NHS implementations shows that perceived organisational support increases when leadership engagement is authentic (Maben et al., 2018).
2. Program Delivery
Regularity matters. Monthly sessions create predictability and build cumulative impact. Irregular delivery weakens engagement.
Use authentic cases. Real scenarios drive emotional connection and relevance. Hypothetical cases rarely produce the same depth of reflection.
Enforce ground rules. Confidentiality, non‑judgement and focus on experience are essential. Facilitators should intervene when discussions drift into blame or problem solving.
Encourage multidisciplinary participation. Invite a mix of clinical staff, administrators, support services and leadership. Diversity enriches perspectives and reduces “us versus them” dynamics.
3. Embed and Evaluate
Integrate insights. Document themes from each session and feed them into risk management and quality improvement processes. Use them to inform training, policy changes and resource allocation.
Provide follow‑up support. Emotional disclosure can surface unresolved strain. Ensure that participants have access to Employee Assistance Programs, peer support, supervision or counselling.
Monitor participation and themes. Track attendance and thematic trends to identify emerging risks and measure program impact. Consider collecting anonymised feedback on psychological safety and perceived benefits.
Celebrate and communicate success. Share stories of how Rounds have led to improvements. Highlight successes to sustain engagement and demonstrate leadership commitment.
4. Limitations and Considerations
Schwartz Rounds are not a standalone solution.
They do not directly change work design. They identify and process experience, but structural issues such as workload or role clarity must be addressed through separate controls.
They depend on facilitation quality. Poor facilitation can undermine safety and reduce participation.
They are also culture-dependent. In low-trust environments, uptake may be limited. However, consistent implementation can contribute to gradual cultural improvement (Grey et al., 2017).
Importantly, Schwartz Rounds function as a supporting control, not a primary one. ISO 45003 makes clear that psychosocial risks must be addressed through changes to how work is designed, managed, and supported.
Case Examples and Lessons Learned
National Health Service (UK)
The UK’s National Health Service (NHS) has implemented Schwartz Rounds across over 140 organisations. Evaluation findings showed that Rounds improved coping with emotional demands, increased perceived organisational support and enhanced psychological safety. Participants reported feeling less isolated and more connected to colleagues across disciplines. The NHS case demonstrates that large, high‑pressure systems can successfully integrate reflective practice when leadership backs the program and ensures facilitator training.
Healthcare Network in the United States
An integrated healthcare network in the U.S. introduced Schwartz Rounds alongside other psychosocial risk controls. Over three years the program facilitated more than 60 sessions. Qualitative data showed improved empathy across professional groups: physicians gained insight into pressures faced by support staff; administrative teams better understood clinical decision‑making; hierarchical barriers softened. The organisation reported improved teamwork, reduced “us versus them” dynamics and higher retention among early‑career staff. Leaders framed Rounds as part of their risk management strategy, not merely a wellbeing initiative, enabling cross‑functional buy‑in and sustained funding.
Cancer Care Centre
Cancer care environments involve sustained exposure to trauma, loss and family distress. A 2021 study in a cancer centre found that Schwartz Rounds reduced compassion fatigue, helped staff restore emotional connection and improved coping with difficult interactions[6]. Participants described re‑engaging with the meaning of their work and feeling less numb. The case illustrates how structured reflection prevents emotional withdrawal and sustains resilience in high‑exposure roles such as emergency services, regulatory investigations and legal practice.
Virtual Rounds During the Pandemic
The NJNEW Virtual Schwartz Rounds provide an example of adaptation during crises. When in‑person sessions were impossible, the institute quickly shifted online, maintaining essential features such as trained facilitators, real cases and confidentiality. Within three years the program reached thousands of nurses[15]. Surveys show that participants value the anonymity and accessibility of virtual sessions and that virtual participation complements self‑care and community support[21]. The success of virtual Rounds suggests that organisations can extend psychosocial support beyond physical boundaries and offer flexible modalities.
Strategic Takeaways
Make the invisible visible. Schwartz Rounds uncover emotional load, ethical tension and cultural signals that traditional risk assessments miss. Once visible, these pressures can be managed.
Integrate with risk management. Reflective forums should inform hazard identification and control measures. Organisations should treat them as part of their psychosocial risk strategy, not as optional wellness extras.
Invest in facilitation and leadership. Skilled facilitation and genuine leadership engagement are non‑negotiable. Leaders who attend and listen send a powerful message about organisational values.
Cultivate psychological safety. Normalising vulnerability and reducing stigma around help‑seeking enhances psychological safety. Higher psychological safety improves reporting, learning and innovation.
Diversify support modalities. Virtual Rounds and complementary programs acknowledge that workers use multiple strategies to maintain well‑being. Providing varied options respects individual preferences and logistical constraints.
Conclusion
The rise of psychosocial injuries and new regulatory requirements demand that organisations move beyond superficial wellness initiatives. Schwartz Rounds offer a pre‑event psychosocial risk management strategy that addresses the emotional and moral burdens of work before they manifest as harm. By providing structured, facilitated forums for collective reflection, Rounds reduce psychological distress, mitigate moral injury, strengthen psychological safety and improve team cohesion. Research shows that the benefits are substantial and cumulative[19]. Virtual adaptations and integration with risk management processes further extend their reach and impact. In high‑pressure environments the question is no longer whether organisations can afford to invest in such programs, but whether they can afford not to.
As psychosocial risk regulation tightens and workers demand safer, more supportive workplaces, interventions like Schwartz Rounds will become integral to organisational strategy. They remind us that risk management is not just about preventing accidents but about honouring the human side of work. When we make space for compassion, connection and honest reflection, we not only protect people – we build stronger, more resilient organisations.
References:
[1] [9] U.S. Work-Related Stress in 2025: Key Stats & Solutions | Wellhub
[2] [10] [21] [22] [23] Workplace Support Engagement and External Help‐Seeking Among Nurses Participating in Virtual Schwartz Rounds: Findings From a Cross‐Sectional Survey
[3] oup.silverchair-cdn.com
https://oup.silverchair-cdn.com/article-minimal/8524092
[4] [5] [8] - Psychosocial hazards | Safe Work Australia
[6] [7] [24] [25] [26] [27] [28] [29] [30] [31] Psychosocial Risk Review
[11] [12] [13] [18] [19] [20] theschwartzcenter.org
https://www.theschwartzcenter.org/media/Schwartz-Rounds-Research-Summary-and-Chart-2024.pdf