
Psychosocial Hierarchy of Controls: What It Means for Your Workplace
Pre-Event Psychosocial Risk Management Framework 8

Introduction
According to the World Health Organization (World Health Organization, 2025), depression and anxiety alone cost the global economy roughly US$1 trillion each year in lost productivity. The International Labour Organization (International Labour Organization, 2026) estimates that psychosocial risks at work factors such as excessive workloads, job insecurity, bullying and unfair systems contribute to around 840,000 deaths annually and 45 million disability‑adjusted life years, with associated economic losses equivalent to 1.37 % of global GDP. In Australia the problem is evident in workers’ compensation data: mental‑health injuries now account for 10.5 % of all serious claims, representing a 97 % increase over the last decade. These claims take more than five times longer to resolve than physical injuries. Such statistics highlight both human suffering and a significant productivity challenge. In response, occupational health and safety systems are expanding beyond physical hazards to address psychosocial hazards stresses arising from how work is designed, organized and experienced.
Central to this evolution is the psychosocial hierarchy of controls (Psychosocial Hierarchy of Controls). Adapted from the classic hierarchy of controls used for physical hazards, the P‑HoC provides a prioritised decision‑making framework for addressing psychosocial risks. Rather than relying on individual resilience or after‑the‑fact counselling, the P‑HoC emphasises eliminating or redesigning the underlying conditions that generate workplace stress. This report offers an in‑depth exploration of the P‑HoC: its origins, underlying rationale, evidence base, criticisms and the regulatory landscape in which it operates. It draws upon research, governmental guidance and industry examples to illustrate how organisations can move from reactive, individual‑level interventions to systemic change.
Origins and Rationale
The Traditional Hierarchy
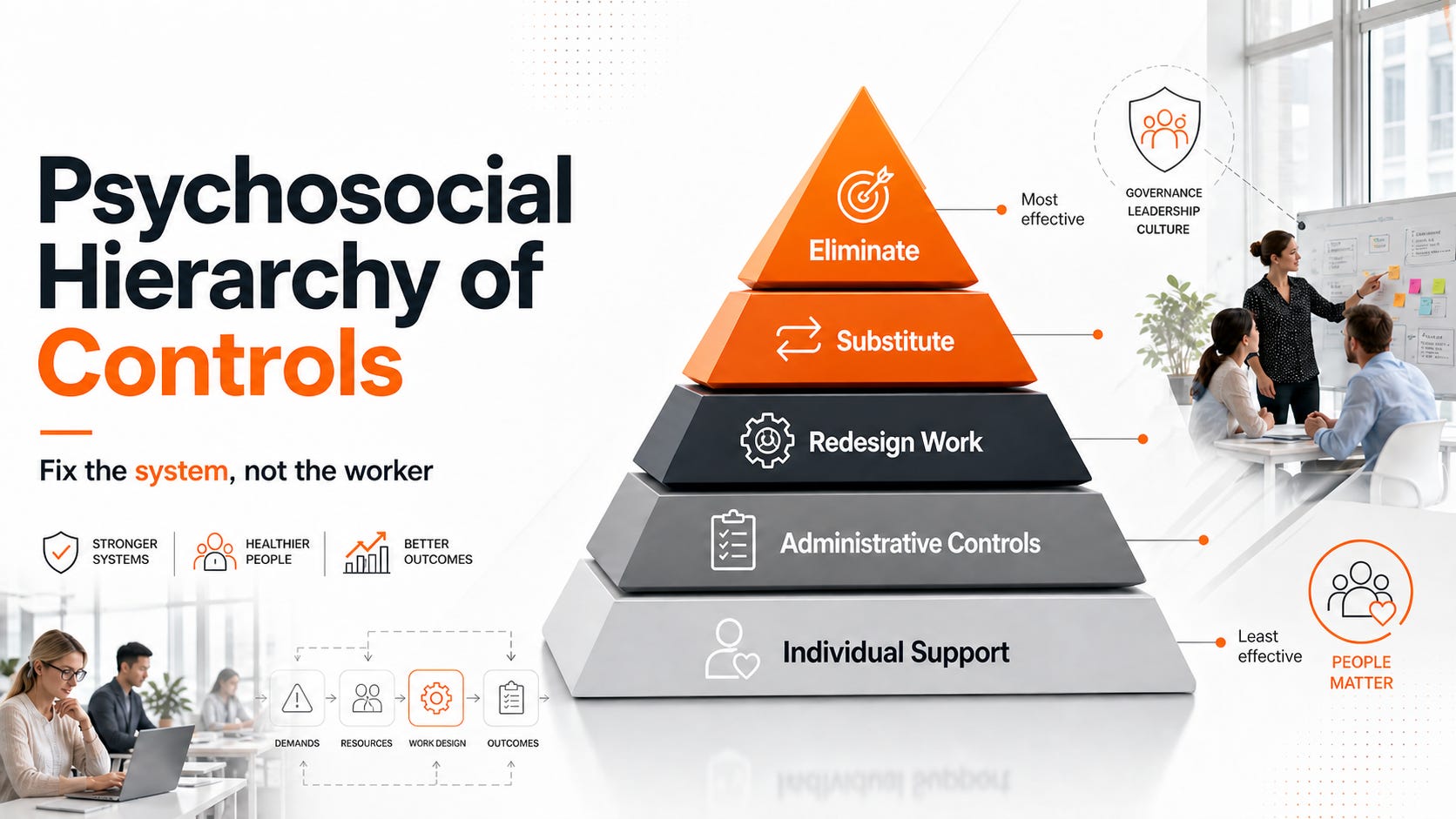
The traditional hierarchy of controls (HoC) is a staple of occupational health and safety. Developed in the mid‑20th century, it ranks hazard control methods from most to least effective: elimination, substitution, engineering controls, administrative controls and personal protective equipment (PPE). The logic is that removing a hazard entirely offers greater protection than merely equipping workers with PPE. For decades this model guided risk management primarily in relation to physical hazards.
Adapting the Model for Psychosocial Risks
As regulators and researchers recognised that mental health injuries and psychosocial disorders were rising, they looked to the HoC for guidance. The NIOSH Total Worker Health® (NIOSH, 2024) hierarchy of controls was one of the first major adaptations. NIOSH’s model sought to integrate health promotion with hazard control by adding organisational and well‑being elements. It prioritises eliminating and substituting unhealthy working conditions, redesigning work environments, educating workers and finally encouraging individual behaviour change. This model emphasises that controlling hazards at the source (policies and work design) is more effective than relying on personal coping strategies.
In 2025, researchers from Denmark’s National Research Centre for the Working Environment expanded the TWH model to develop the Psychosocial Hierarchy of Controls (Psychosocial Hierarchy of Controls). Their study, which examined interventions across nine Danish companies addressing bullying, unclear demands and high workload, underscored that elimination and organisational redesign were more effective than individual measures. The researchers proposed levels akin to the physical HoC but tailored to psychosocial hazards: (1) eliminate hazardous working conditions; (2) substitute with healthier practices; (3) re‑engineer the work environment; (4) administrative controls; and (5) personal change/support. They emphasised that combining interventions across levels yields the best results.
Another innovation, the Work Systems Hierarchy of Controls (WS‑HoC), emerged from Australian human‑factors researchers. Noting that many psychosocial risks arise from systems of work rather than discrete hazards, they added a new level called “re‑design work systems” between elimination and individual actions. This level encourages employers to redesign job tasks, management practices and organisational structures. The WS‑HoC aims to prevent effective redesign strategies from being misclassified as lower‑order administrative controls and thus overlooked.
Both models maintain the principle that elimination of hazards such as reducing unreasonable workloads or stopping bullying remains the priority. They acknowledge, however, that psychosocial hazards are complex, multi‑causal and sometimes intangible; therefore, elimination may be challenging and often requires broader organisational change rather than removal of a discrete hazard.
Framework: Levels and Examples
The P‑HoC is best understood by examining each level. The following sections explain the intention behind each tier and provide examples drawn from industry guidance and case studies.
1. Eliminate Hazardous Conditions
Elimination involves removing the psychosocial hazard entirely. For physical risks this might mean removing a toxic substance; for psychosocial risks it could mean removing unreasonable performance demands or stopping abusive behaviours. The Danish study found that hiring additional staff or restructuring work to reduce workload had a major impact on psychosocial well‑being. Similarly, the Canadian Mental Health Association’s People Working Well BC network suggests involving hotel employees in co‑designing their job roles to address inefficiencies and dissatisfaction. By eliminating poor work design and giving workers control over schedules, this intervention reduces stress at its source.
Regulatory guidance underscores elimination. Queensland’s Managing the Risk of Psychosocial Hazards at Work Code of Practice requires duty holders to eliminate psychosocial risks so far as reasonably practicable. SafeWork NSW stresses that improving work design, such as distributing workloads fairly and clarifying roles – effectively addresses root causes. Law firms and consulting companies have taken elimination seriously by cutting back billable hour targets and capping overtime. While formal case studies are scarce, reducing targets addresses the hazard (chronic overwork) directly rather than treating its consequences.
2. Substitute Unhealthy Practices
Substitution involves replacing hazardous processes with safer ones. In psychosocial contexts this may mean replacing rigid schedules with flexible hours, introducing job rotation or substituting manual reporting with automated systems. The Danish P‑HoC described substituting harmful practices with those promoting mental health, such as job rotation and flexible working. At a museum that lacked safety communication, People Working Well BC recommended redesigning communication processes by instituting regular briefings and clear reporting channels, thereby substituting haphazard communication with a structured system. These substitutions change processes rather than adding new tasks, making them durable and scalable.
3. Re‑engineer or Redesign the Work Environment
Engineering controls, in psychosocial terms, translate to redesigning the physical or organisational environment to reduce stress. Examples include restructuring teams to enhance collaboration, improving ergonomics, controlling noise and lighting, or training managers to model respectful behaviours. In the People Working Well BC example, a restaurant experiencing tension and conflict implemented leadership training and a formal conflict‑resolution process to foster a supportive culture. The P‑HoC aligns this level with the TWH principle of redesigning the work environment for safety and well‑being, emphasising management support and systemic adjustments rather than one‑off training.
Other examples include providing restorative spaces, adjusting shift patterns to reduce fatigue, and designing tasks to allow recovery. The ILO notes that alternating cognitively intense tasks with less strenuous activities, limiting complexity and rotating staff to less demanding roles can mitigate psychosocial risks. Such redesign acknowledges that the work environment, physical and social, profoundly influences mental health.
4. Administrative Controls
Administrative controls encompass policies, procedures, training and communication aimed at reducing exposure. They are less effective than elimination or redesign because they rely on individuals adhering to rules, yet they remain necessary to support higher‑order controls. The P‑HoC positions administrative measures – such as psychological health policies, stress management programmes and clear reporting procedures – on the fourth tier. People Working Well BC recommends developing a psychological health and safety policy with worker input to address stressors such as dealing with aggressive customers and long shifts. Queensland’s mandatory sexual harassment prevention plans require employers to identify risks, outline controls and document consultation and reporting procedures.
Administrative controls also include training managers to recognise signs of burnout, establishing fair performance review processes, and communicating expectations. They can be particularly useful when elimination is impractical; however, they should not be the sole response. The SafetyInsights review warns that organisations often default to administrative or individual‑level measures because they are easier and cheaper to implement, even though evidence suggests they are less effective in addressing root causes.
5. Personal Change and Support (Individual Measures)
At the base of the hierarchy are interventions targeted at individuals, such as mindfulness training, employee assistance programmes (EAPs), counselling and stress management workshops. These measures can improve coping skills, but they do not remove the hazard. The P‑HoC treats personal change and support as supplementary measures to complement organisational interventions. SafetyInsights emphasises that individual interventions often have stronger evidence because they are easier to study and implement, yet they may not address the primary drivers of a healthy psychosocial environment. The OHS Reps also caution against relying on EAPs and resilience training without addressing systemic factors.
Combining Controls
Most workplaces require a combination of controls. The Danish study highlighted that the best outcomes arose from using comprehensive organisational and individual measures across multiple levels. For example, when addressing bullying, eliminating the behaviour through clear anti‑bullying policies (administrative) and accountability mechanisms (elimination) should be coupled with training to improve interpersonal skills (engineering) and counselling for affected workers (personal support). Effective psychosocial risk management is iterative; controls must be implemented, evaluated and adjusted over time.
Evidence and Effectiveness
Organisational vs Individual Interventions
Systematic reviews show that organisational‑level interventions can prevent stress and improve well‑being, but they often do not achieve their intended outcomes. This inconsistency arises because organisations are complex systems; factors such as leadership commitment, organisational culture, and implementation quality influence success. Studies indicate that interventions aiming to reduce workload or increase resources – such as adjusting staffing levels, altering shift patterns, or providing more autonomy over scheduling, have positive effects. However, these interventions require significant resources and may challenge existing business models; as a result, employers are sometimes reluctant to adopt them.
Evidence for individual‑level interventions is more consistent because these programmes (e.g., mindfulness, resilience training) are easier to deliver and evaluate. They can improve psychological outcomes, yet they address symptoms rather than root causes. The P‑HoC authors argue that organisational interventions should remain the core focus because prevention through system design benefits all workers, whereas personal change primarily benefits those receiving the intervention.
Case Study: Danish “Agreement to Problem‑Solve”
The Danish study underpinning the P‑HoC evaluated interventions in nine companies participating in the “Agreement to Problem‑Solve” labour inspection programme. Companies addressed issues such as bullying, unclear demands and high workloads. Interventions high on the hierarchy, such as hiring new staff and restructuring work, yielded a significant positive impact on the psychosocial environment. Equally important was the finding that a combination of organisational and individual measures delivered the best outcomes. This demonstrates that while elimination and substitution should be prioritised, lower‑order measures can complement and strengthen overall interventions.
Work Systems Hierarchy Application
Researchers tested the Work Systems Hierarchy of Controls by analysing 79 risk controls developed to reduce musculoskeletal and psychosocial hazards among paramedics. Most controls were classified under the “re‑design work systems” level, highlighting the importance of work redesign as a control measure. The study concluded that clear definitions and guidance are essential to ensure that effective system‑level controls are not misclassified as mere administrative measures and discounted.
Trust as an Indicator of Effective Controls
An often overlooked aspect of psychosocial interventions is trust. An insightful commentary notes that trust is not itself a psychosocial control but an outcome reflecting whether controls are credible and properly implemented. Psychosocial hazards include excessive workload, poor role clarity, inadequate leadership, bullying and job insecurity. Controls must change underlying conditions through work design, management practices, organisational systems and interpersonal dynamics; policies without behavioural change will fail. Trust emerges when organisations acknowledge problems, make transparent decisions, act consistently, and continuously monitor implementation. Organisations can use trust as a leading indicator of the effectiveness of their psychosocial controls.
Critiques and Nuances
Misalignment With Physical Hierarchy
While adapting the physical HoC provides a useful starting point, some experts argue that psychosocial hazards differ fundamentally from physical hazards. Skodel notes that the traditional hierarchy does not align neatly with psychosocial controls. It emphasises the difference between preventive controls (work design) and reactive controls (support services) and urges organisations to consider the effort, resources and impact of each intervention. Psychosocial controls often require cultural and systemic change, which may not fit into a rigid hierarchy of substitution and engineering.
Evidence Limitations and Implementation Challenges
The SafetyInsights article points out that the evidence base for organisational‑level interventions is weaker than for individual programmes, not because they are ineffective but because they are harder to study and implement. Organisational interventions must contend with complex contexts, and success depends on leadership commitment, staff engagement and resources. As a result, many organisations prefer administrative or individual interventions, which are easier to implement and can serve the purpose of “demonstrated safety” appearing to take action without tackling root causes. This can lead to “tick‑box” compliance, where employers provide resilience training or EAPs but fail to eliminate excessive workloads or toxic cultures.
Complexity of Psychosocial Risks
Psychosocial hazards arise from the interaction of work design, organisational culture, leadership, social relationships and individual differences. They can be chronic and cumulative (e.g., long‑term workload imbalance) or acute (e.g., exposure to traumatic events). Multiple hazards can interact to increase risk. Because psychosocial hazards are often intangible and subjective, it can be challenging to assess their severity and to decide what constitutes reasonable elimination. For example, some forms of stress (e.g., during peak business periods) may be intrinsic to a role. The P‑HoC acknowledges this nuance by advocating for combined controls rather than rigid adherence to elimination when it is impractical.
Work Design vs Personal Responsibility
Critiques also focus on the moral hazard inherent in focusing on individual coping. Skodel warns that organisations often implement “reactive” measures like mindfulness sessions while neglecting workload and role clarity. OHS Reps admonish employers not to jump straight to EAPs and resilience training; instead, they should document why lower‑tier controls are chosen and review effectiveness over time. There is a risk that emphasising personal resilience implicitly blames workers for failing to cope rather than addressing the organisational causes of stress.
Need for Clear Definitions and Guidance
The WS‑HoC authors note that misclassifying effective system redesign controls as administrative measures can lead to them being discounted. Clear definitions and classification criteria are needed to avoid confusion and ensure that controls are prioritised appropriately. Without clear guidance, different practitioners may place the same intervention at different levels, undermining the hierarchy’s usefulness as a decision‑making tool.
Integration With Total Worker Health
There is debate over whether an entirely new hierarchy is necessary or whether psychosocial risks can be addressed through an integrated HoC. An opinion piece in OHS Canada argues for a combined framework that integrates insights from the P‑HoC and TWH into the classic HoC. The authors emphasise expanding the substitution level beyond replacing hazardous substances to include redesigning work systems and organisational structures. They advocate broadening engineering controls to encompass environmental and psychosocial modifications and redefining the bottom tier as “Individual actions/PPE”, highlighting that individual resilience is a supportive element rather than a substitute for organisational change. This integrated model encourages practitioners to consider multiple levels simultaneously and fosters innovation in risk management.
Regulatory Landscape
Australia
Australia has been at the forefront of legislating psychosocial risk management. Queensland’s framework is particularly robust. The Work Health and Safety (Sexual Harassment) Amendment Regulation 2024 introduced express obligations to manage psychosocial hazards, with mandatory written prevention plans for sexual harassment taking effect on 1 March 2025. Plans must identify risks, set out control measures following the hierarchy of controls, document consultation and reporting processes, and be reviewed at least every three years. Queensland’s Code of Practice provides detailed guidance on work design, systems thinking and the use of tools like the Psychosocial Hazard Work Re‑Design Tool (PHReD‑T). It emphasises eliminating psychosocial risks where reasonably practicable and improving work systems.
In Victoria, the Occupational Health and Safety (Psychological Health) Regulations 2025 came into force on 1 December 2025. Employers are now explicitly required to identify psychosocial hazards, take reasonable steps to eliminate or control associated risks, and review controls. The regulations emphasise that psychological injuries can be as harmful as physical ones. Employers must consult health and safety representatives and update systems to meet compliance. Unlike earlier drafts, the final regulations do not require mandatory reporting of psychosocial complaints; however, WorkSafe published templates to assist with risk assessments. Importantly, the regulations implement a modified hierarchy of controls, making it clear that training and information cannot be relied on unless higher‑order controls are not reasonably practicable. They also broaden the definition of psychosocial hazards to include work design, systems and personal interactions.
New South Wales, under SafeWork NSW, requires duty holders to eliminate psychosocial risks so far as reasonably practicable and to consider how hazards and risks may interact. Guidance emphasises systems thinking and work design as primary controls. The WHS Regulation 2025 (NSW) and the Code of Practice: Managing Psychosocial Hazards at Work 2021 provide detailed instructions for identifying hazards, determining control measures and using tools like PHReD‑T. Duty holders must assess the dynamic relationships within the work system and design safe systems of work accordingly.
International
Globally, regulators are increasingly adopting psychosocial risk management frameworks. ISO 45003:2021, part of the ISO 45000 series, offers guidelines for managing psychosocial risks within occupational health and safety management systems. It encourages organisations to integrate psychological health into their OH&S management systems, addressing hazards such as role ambiguity, workload imbalance and poor communication. ISO 45003 is not a certifiable standard but provides guidance that complements ISO 45001 and encourages organisations to address psychosocial risks proactively. Risk training providers emphasise that effective psychosocial risk management can reduce absenteeism, improve engagement and foster supportive cultures.
In New Zealand, WorkSafe’s 2025 Managing Psychosocial Risks at Work Guidelines emphasise identifying psychosocial risks, assessing and prioritising them like physical hazards, implementing controls and monitoring and reviewing effectiveness. The guidance warns that psychosocial risks are not reduced by “nice‑to‑have” well‑being initiatives but by redesigning work and considering impacts on physical and mental health. Employers are reminded that under New Zealand’s Health and Safety at Work Act (HSWA), they have a duty to manage both physical and psychological risks.
The ILO and WHO have reinforced the need for psychosocial risk management globally. The ILO’s 2024 report on the psychosocial working environment notes that long working hours, job insecurity and workplace harassment contribute to cardiovascular diseases and mental disorders, with annual economic losses of 1.37 % of global GDP. The WHO’s Mental Health Atlas highlights the US$1 trillion productivity cost of depression and anxiety. These organisations urge governments to intensify investment, reform laws, expand community‑based care and integrate mental health into primary care. Such guidance underpins regulatory trends and emphasises that psychosocial risk management is a global public health priority.
Metrics and Measurement
Effective psychosocial risk management requires robust measurement. Organisations should track both process measures (e.g., distribution of controls across the hierarchy) and outcome measures (e.g., levels of stress, absenteeism, turnover). Key metrics include:
1. Distribution of controls: Document how many interventions fall at each level of the P‑HoC. For example, track whether interventions focus on elimination (e.g., workload reduction), substitution (e.g., job rotation), redesign (e.g., ergonomic improvements), administrative controls (e.g., policies) or individual support (e.g., EAP usage). The SafetyInsights article notes that organisations often overemphasise administrative and individual interventions; measurement can reveal such imbalances.
2. Hazard exposure: Assess the prevalence and severity of psychosocial hazards through surveys and qualitative feedback. Common hazards include high job demands, low job control, role ambiguity, interpersonal conflict and poor organisational justice. Instruments like the Copenhagen Psychosocial Questionnaire and other validated tools can be used.
3. Health and productivity outcomes: Track mental health claims, stress‑related absence and return‑to‑work durations. In Australia, mental health claims accounted for 10.5 % of all serious workers’ compensation claims in 2022–23, representing a 97 % increase over a decade. Monitoring trends helps evaluate whether controls are reducing risk.
4. Leading indicators: Measure trust in management, perceptions of fairness, psychological safety and employee engagement. Trust, as previously noted, is a leading indicator of successful psychosocial controls. Regular climate surveys can capture these indicators.
5. Review and feedback mechanisms: Document how often controls are reviewed and updated. Regulatory guidance requires employers to review controls after organisational changes, new information, reported psychological injuries or evidence that existing measures are inadequate.
Practical Guidance for Implementation
Leadership Commitment and Risk Management Expertise
Effective psychosocial risk management demands leadership support. Senior leaders must champion mental health by allocating resources, setting realistic performance expectations and modelling positive behaviours. Risk management expertise is required to identify hazards, assess risk and select appropriate controls. Government guidance encourages employers to consult health and safety representatives and involve workers throughout the process. This participation fosters buy‑in and ensures interventions address real issues rather than perceived problems.
Systemic Work Design
The work design approach emphasises designing or redesigning work tasks, processes and environments to reduce psychosocial risks. SafeWork NSW advocates using systems thinking to examine how different parts of the work system interact. Tools like PHReD‑T guide managers in redesigning tasks, reallocating duties, adjusting shift patterns and altering staffing. Work redesign may involve reducing workloads, clarifying roles, increasing autonomy, improving ergonomics, or changing the physical environment. For example, alternating cognitively demanding tasks with less strenuous activities and allowing sufficient recovery time can mitigate mental fatigue.
Combined and Sequential Interventions
The hierarchy should not be interpreted rigidly; multiple controls can and should be implemented concurrently. Skodel advises combining major interventions (e.g., redesigning job structures) with minor interventions (e.g., training) and spacing them out to avoid overwhelming employees. Organisations should document the rationale for using lower‑tier controls and ensure they complement rather than substitute higher‑order measures. Continuous monitoring and evaluation are essential to assess effectiveness and adjust interventions.
Avoiding Pitfalls
1. Do not default to EAPs and resilience training. These programmes can support individuals but should not be the primary control. Organisations must avoid blaming workers for failing to cope.
2. Document decisions. When higher‑level controls are not practicable, document why and demonstrate that elimination and substitution were considered.
3. Integrate physical and psychological health. The People Working Well BC article stresses considering physical and psychological aspects simultaneously. Work design that reduces physical strain often reduces psychosocial stress too; for instance, improved ergonomics may reduce musculoskeletal pain and associated anxiety.
4. Be transparent and build trust. Communicate openly with workers about hazards, decisions and progress. Acknowledge failures and successes. This transparency builds trust, which is critical for effective psychosocial interventions.
When to Use the P‑HoC
The hierarchy is most useful when deciding how to control psychosocial hazards after they have been identified. Regulators and researchers emphasise starting at the top – elimination – and working down only when higher‑order controls are not reasonably practicable. Because psychosocial hazards often have complex causes, the P‑HoC serves as a reminder to prioritise systemic solutions rather than quick fixes. It is particularly relevant when designing new work systems, responding to emerging risks (e.g., remote work, AI), or updating policies after incidents. Employers should also use the hierarchy when developing mandated prevention plans, such as Queensland’s sexual harassment plans.
Case Examples
Hospitality Sector: Work Design and Culture
In the tourism and hospitality sector, psychosocial hazards such as low autonomy, aggressive customers and long shifts are common. The People Working Well BC network illustrates how the P‑HoC can be applied:
Elimination: A hotel identified that employees had little input into job design and shift scheduling. Management instituted a structured job design framework where staff co‑designed workflows and schedules and established a feedback loop to continuously assess and adjust. This eliminated the hazard of insufficient worker input and improved morale.
Substitution: A museum improved its communication by instituting regular safety briefings and clear reporting channels. By substituting ad‑hoc communication with structured processes, staff stress and unaddressed hazards decreased.
Engineering: A restaurant faced frequent interpersonal conflicts. Training managers to model respectful behaviour and implementing a conflict‑resolution process improved the work culture.
Administrative: A pub developed a psychological health and safety policy with staff input and created procedures for dealing with difficult customers.
Individual Support: A ski resort provided mental health resources, encouraged managers to model healthy behaviours and limited overtime.
Emergency Services: Paramedics
Musculoskeletal and psychosocial injuries are prevalent among paramedics due to high workloads, shift work and exposure to trauma. Applying the Work Systems Hierarchy, researchers categorised 79 risk controls developed by paramedics. Most controls fell within the re‑design work systems level, such as redesigning shift patterns, introducing mechanical lifting aids to reduce physical strain and changing dispatch procedures to distribute workload more evenly. The study emphasised that work redesign – not just individual training is critical to reducing both physical and psychosocial risks. It concluded that clear definitions can prevent misclassification of these controls as mere administrative measures.
Law Firms: Reducing Billable Hours
Although specific case studies are limited in the literature, the legal profession is an illustrative example. High billable‑hour targets, long working hours and adversarial cultures contribute to high rates of burnout and mental ill‑health among lawyers. Proactive firms have experimented with elimination strategies, such as reducing billable hour expectations and instituting mandatory disconnect periods. Others have introduced flexible schedules (substitution), team‑based workflows (redesign) and policies against after‑hours emails (administrative). These measures are aimed at addressing root causes rather than offering yoga classes or mindfulness sessions.
Remote Work and Digitalization
The rise of remote work, digital technologies and AI brings new psychosocial risks such as technostress, isolation and constant connectivity. The ILO notes that digitalisation and new work arrangements contribute to higher levels of psychosocial risks. Employers can apply the P‑HoC by eliminating unnecessary digital notifications, substituting synchronous communication with asynchronous platforms to allow flexibility, redesigning workflows for remote collaboration and establishing policies that respect boundaries. Individual support, such as training workers in digital literacy and providing counselling for technostress, should supplement systemic changes.
Integration With Broader Well‑Being Strategies
Total Worker Health and Holistic Models
The P‑HoC aligns with the Total Worker Health philosophy, which integrates protection from work‑related hazards with promotion of overall well‑being. NIOSH’s TWH hierarchy emphasises elimination, substitution, redesign, education and encouragement. Both models highlight that hazard elimination and redesign provide the greatest benefits, while educational and individual behaviour change should support, not replace, systemic interventions. Integrating psychosocial controls within existing OH&S management systems (e.g., ISO 45001) ensures alignment with broader risk management processes.
Organisational Culture and Psychological Safety
Psychological safety – the belief that one can speak up without fear of negative consequences is a critical component of psychosocial well‑being. Controls that create a supportive culture, encourage open dialogue and empower employees to report issues contribute to elimination and redesign. Training managers in empathetic leadership, establishing clear procedures for reporting harassment, and embedding mental health in performance metrics can all reinforce a culture of safety. When workers trust their employer’s commitment to mental health, they are more likely to engage with controls and provide honest feedback.
Intersection With Physical Health
Psychosocial and physical hazards often share underlying causes. High workloads, for example, can cause both stress and musculoskeletal injuries. Conversely, musculoskeletal pain can increase psychological stress. SafeWork NSW notes that many psychosocial and physical hazards emerge from the same work system issues. Integrating control measures across physical and psychosocial domains can achieve synergies; improving ergonomics may reduce both physical strain and frustration, while reducing overtime can decrease fatigue and stress. This holistic view supports the “whole‑person safety” approach championed by some practitioners.
The Bigger Picture: Duty and Opportunity
The P‑HoC operationalises the duty of employers to eliminate or minimise risks so far as reasonably practicable, as required by work health and safety laws. It shifts the focus from reactive, individual treatment to proactive, systemic risk management. Addressing psychosocial hazards is not just about compliance; it offers opportunities to enhance productivity, reduce turnover, improve reputation and support sustainable development. The ILO emphasises that improving the psychosocial working environment strengthens productivity and organisational performance.
However, realising these benefits requires meaningful action. Employers must invest in work redesign, leadership development, monitoring and continuous improvement. Governments should provide clear guidance, robust enforcement and support for small businesses. Researchers should continue to evaluate the effectiveness of organisational interventions and develop practical tools for assessment and redesign. Finally, workers and unions must remain vigilant advocates for safe and healthy work systems.
Conclusion
The psychosocial hierarchy of controls represents a significant evolution in occupational health and safety. By prioritising elimination and redesign of hazardous work conditions, it addresses the root causes of work‑related stress and mental ill‑health. Evidence from the Danish P‑HoC study, the Work Systems Hierarchy application and regulatory guidance demonstrates that systemic interventions yield meaningful improvements, especially when combined with supportive policies and individual resources. Yet challenges remain: evidence for organisational interventions is still developing, implementation can be complex and costly, and some employers continue to favour lower‑order controls for convenience.
To navigate these challenges, organisations should adopt a systems‑thinking approach, involve workers in decision‑making, measure and review controls, and embed psychosocial risk management within broader health and safety systems. Regulators should refine guidance and classification criteria, while researchers must continue investigating what works. Ultimately, the P‑HoC is more than a checklist; it is a strategic framework that, when applied thoughtfully, can transform workplaces into environments where mental and physical health flourish.
References
1. Kjærgaard, A., Rudolf, E. M., Palmqvist, J., Jakobsen, M. E., & Ajslev, J. Z. N. (2025). The psychosocial hierarchy of controls: Effectively reducing psychosocial hazards at work. American Journal of Industrial Medicine, 68(3), 250–263. Summary via SafetyInsights.
2. People Working Well BC. (2026). Leveraging the physical hierarchy of controls for psychological hazard management. Canadian Mental Health Association. Examples of elimination, substitution and other controls.
3. Skodel. (2025). Preventive vs reactive psychosocial controls in the workplace. Skodel Blog. Highlights that work design controls have different levels of impact.
4. OHS Reps. (2025). Do we need a new hierarchy of controls for psychosocial hazards? Victorian Trades Hall Council. Discusses the Work Systems Hierarchy of Controls.
5. OHS Reps. (2025). Danish study optimises hierarchy of controls for psychosocial hazards. Victorian Trades Hall Council. Summarises a Danish intervention study and its findings.
6. Total Worker Health – CDC. (2024). Hierarchy of controls applied to Total Worker Health®. Centers for Disease Control and Prevention. Describes elimination, substitution, redesign, education and individual encouragement.
7. OHS Canada Magazine. (2025). Rethinking the hierarchy of controls: A comprehensive framework for modern workplace hazards. Highlights integrating physical and psychosocial controls and redefining levels.
8. WorkSafe Victoria. (2025). New regulations make psychological health a priority. WorkSafe Victoria media release. Announces regulations requiring employers to eliminate or control psychosocial hazards.
9. DLA Piper. (2025). Victoria: New psychosocial health regulations for employers now in force. Summarises duties to identify, assess and control psychosocial hazards and introduces a modified hierarchy of controls.
10. SafeWork NSW. (2024). Designing work to manage psychosocial risks. Provides guidance on work design and systems thinking.
11. Mibo Work. (2025). Psychosocial hazards QLD: Compliance guide. Describes mandatory sexual harassment prevention plans and hierarchy of controls.
12. WorkSafe Queensland. (2025). Updated guidance: managing workplace psychosocial risks. Outlines risk management processes and defines psychosocial hazards.
13. WHO. (2025). Over a billion people living with mental health conditions – services require urgent scale‑up. Reports that depression and anxiety cost the global economy US$1 trillion each year.
14. ILO (as reported by AIHA). (2026). ILO estimates effects of psychosocial risks at work. Notes 840 000 deaths per year and economic losses of 1.37 % of global GDP; emphasises preventive measures.
15. Occupational Medicine (Blog). (2025). Work-related injuries in Australia: A GP’s perspective. Reports that mental health claims account for 10.5 % of serious claims and have increased by 97 % over a decade.
16. Wellbeing First NZ. (2025). Simplifying WorkSafe’s latest psychosocial risk guidelines. Emphasises that psychosocial risks are managed through work design rather than well‑being initiatives and outlines New Zealand guidance.